




 Olivier Chevenement
Olivier Chevenement
MRI is central to preoperative planning for neurological devices. But during the surgery it cannot provide the real-time intraoperative feedback surgeons need once craniotomy, retraction, and brain shift change the anatomy. Intraoperative ultrasound bridges that gap. Here’s what it means for your evidence package.
By Olivier Chevènement, DVM, PhD | Director of Preclinical Veterinary Research, Veranex
If you’re developing a neurological device (a neurostimulator, drug delivery system, shunt, or implantable sensor for example) your preclinical study must prove precise target engagement. MRI excels here as a noninvasive roadmap, revealing cortical/subcortical architecture, lesion boundaries, and landmarks before the procedure begins. But once the animal is positioned, the craniotomy performed, and surgical manipulation underway, brain shift occurs: cerebrospinal fluid redistributes, tissue displaces, and your preoperative map loses spatial accuracy.(1)
This isn’t theoretical. It’s documented in neurosurgical literature and routine in preclinical work we’ve conducted. Standard MRI workflows aren’t available intraoperatively due to magnetic field constraints and OR incompatibility with metallic instruments. Without real-time imaging, you risk protocol deviations, lost data points, or repeat procedures that delay your timeline and burn through budget.
 The most common intraoperative imaging modality is computed tomography (CT), which excels at bone landmarks and stereotactic framing. You can fuse it with preoperative MRI to triangulate targets(¹). But CT lacks soft tissue contrast for confirming device placement, ruling out hemorrhage, or verifying trajectories. CT alone cannot provide those answers in real time.
The most common intraoperative imaging modality is computed tomography (CT), which excels at bone landmarks and stereotactic framing. You can fuse it with preoperative MRI to triangulate targets(¹). But CT lacks soft tissue contrast for confirming device placement, ruling out hemorrhage, or verifying trajectories. CT alone cannot provide those answers in real time.
That’s where ultrasound steps in as a practical, complementary solution.(2)
A practical bridge
Ultrasound is a way to close that gap.
Ultrasound systems are portable, OR-compatible, and provide stereotactic images with minimal distortion.²˒³ Intraoperative brain ultrasound works through craniotomies or small burr holes, using low- or high-frequency probes for different depths, eliminating the need for opening of the dura to obtain quality images.
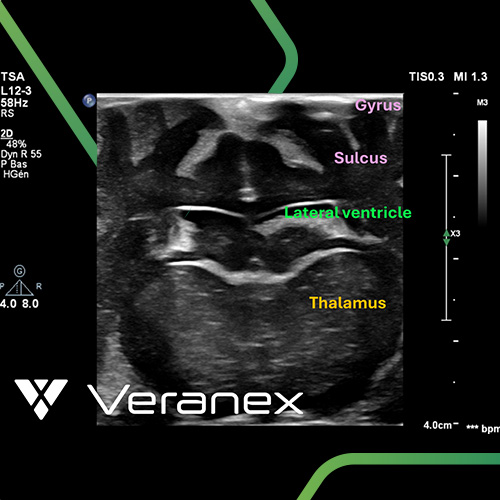
What can you see? Fluid-filled ventricles and cisterns that serve as excellent topographical landmarks.²˒³˒⁴ The boundaries between solid tissue, cyst, and necrosis. Perioperative hemorrhage, acute hematoma formation, and to a lesser extent brain edema around implanted devices.⁵ The technique also allows real-time guided punctures of cyst, mass, and CSF, and safer surgical trajectories. And you can see brain shift itself: real-time, quantitative, while the surgeon can still adjust.¹
Intraoperative brain ultrasound produces two-dimensional images informative and in real-time, but not the full volumetric picture MRI provides. But in the operating room, for the specificity of what your preclinical study needs, ultrasound provides something MRI structurally cannot: spatial intelligence at the moment it matters most.
What this actually changes for your preclinical neuro study
Without intraoperative imaging, your study generates placement data based on what the preoperative MRI predicted and what the postoperative MRI, days later, confirms. If something shifted during the procedure, you may not know until the images come back. If the device is not where it should be, that is a data point lost. That could mean a protocol deviation, a repeated procedure, or an animal that cannot contribute to the dataset your submission requires. For a startup watching its burn rate, every one of those outcomes costs time and money you may not recover. Larger companies face similar risks to timelines and submission packages.
With intraoperative ultrasound, the surgeon knows (during the procedure, not after it) whether the device is positioned correctly, whether there is unexpected tissue response, or whether the trajectory needs adjustment. The answer is available in the moment, while it can still be corrected if needed. Not after days of scheduling and image processing.
The practical result: fewer surprises at the MRI timepoint. Fewer protocol deviations. More confidence that each animal is contributing clean, defensible data to the evidence package your submission depends on. For sponsors, that translates directly into time saved, critical timelines met.
Where this kind of thinking comes from
This is not common in preclinical neurosurgery. Every CRO may have an ultrasound machine. The question is whether the team behind it has the depth of experience to use it this way and the instinct to offer it before you know you need it.
At Veranex, including our industry leading preclinical lab in Paris, this has less to do with equipment than with how our team is built. We are approximately one hundred people, including fifteen veterinarians across specialties. Our background as veterinarians carries multiple skill sets, and because we work together daily, sharing knowledge across cardiovascular, neurological, and musculoskeletal programs, expertise developed in one domain flows naturally into another.
The echocardiographic imaging skills refined over decades of cardiovascular work, across thousands of cardiac procedures, translate directly into neurological applications. When we bring ultrasound into the OR for a novel neuro modality, we are not learning on the fly. We are applying knowledge and connecting specialties to fill a gap most preclinical labs cannot. Applying echocardiographic skills to neuro procedures fills gaps most preclinical labs cannot.
Neurological guidance under ultrasound not only allowed us to visualize the target to reach but also the way tissue got deformed when the device went through!
If you are planning a preclinical neurological study, consider these before the protocol is finalized:
How will you confirm device placement during the procedure, not just before and after it? What is your plan if brain shift compromises the accuracy of your preoperative imaging? Does your CRO have the intraoperative imaging depth to answer in the moment, or will you be waiting days to learn whether the implant landed where it should?
These are not hypothetical questions. They are the difference between a study that generates the evidence you need efficiently, effectively, and with confidence, and one that generates ambiguity you will have to explain.
We have supported a wide range of neurological studies and continue expanding what is possible integrating intraoperative ultrasound alongside MRI, CT, and micro-CT within individual programs to build the evidence packages our sponsors' submissions require. Every capability we develop aims to make our sponsors' work go faster and further.
Many of the sponsors who have worked with us say it was worth the trip. You could be next!

Partner with Proven GLP Studies Excellence
At Veranex, we've guided hundreds of medical device companies through successful preclinical programs over 25+ years. Our Atlanta and Paris labs combine purpose-built GLP facilities with deep therapeutic area expertise across cardiovascular, neurology, orthopedics, ophthalmology, and regenerative medicine.
With over 3,000 procedures annually and devices now treating 1+ million patients, we bring the strategic insight, model development and surgical expertise to help you avoid costly missteps. Our integrated approach embedded within the industry's only iCRO, means we're partners throughout your journey, not just a testing facility.
We don't just conduct studies. We help you build regulatory strategies that work. Our integrated approach means you have access to preclinical expertise, in-house histopathology, and regulatory guidance all under one roof, precisely when you need it.
If you're evaluating your readiness for GLP preclinical studies or need a partner who can guide you from pilot work through regulatory submission, contact our team today. Let's discuss how we can help you build the right team for preclinical success.

Olivier Chevènement, DVM, PhD, is Director of Preclinical Veterinary Research at Veranex, based in Paris. He specializes in neurological and cardiovascular preclinical research and has led the development of advanced intraoperative imaging protocols across multiple therapeutic areas.
References
- Schulz C, Waldeck S, Mauer UM. Intraoperative image guidance in neurosurgery: development, current indications, and future trends. Radiol Res Pract. 2012;2012:197364. doi:10.1155/2012/197364
- Marinho AM, Barua M, Haller J, Ryken TC. Enhanced anatomic visualization with ultrasound-assisted intracranial image-guidance in neurosurgery. Technol Cancer Res Treat. 2002;1(3):181–186. doi:10.1177/153303460200100303
- Vavruska J, Buhl R, Petridis AK, Maslehaty H, Scholz M. Evaluation of an intraoperative ultrasound training model based on a cadaveric sheep brain. Surg Neurol Int. 2014;5:46. doi:10.4103/2152-7806.130314
- Ray WZ, Barua M, Ryken TC. Anatomic visualization with ultrasound-assisted intracranial image guidance in neurosurgery: a report of 30 patients. J Am Coll Surg. 2004;199(2):338–343. doi:10.1016/j.jamcollsurg.2004.03.019
- Smith SJ, Vogelzang RL, Marzano MI, Cerullo LJ, Gore RM, Neiman HL. Brain edema: ultrasound examination. Radiology. 1985;155(2):379–382. doi:10.1148/radiology.155.2.3885307